
Functional Assessment for Hip Centering
And a helpful Sacroiliac Test because "knowledge is power"

I’ve always been somewhat skeptical of cut-and-dry orthopedic testing. As a young, injury-prone professional modern dancer, I became very familiar with the physiotherapist’s office and its typical assessments. I would repeat the same tests at home and quickly learn how to “pass” them by stretching or strengthening beforehand. I also noticed significant variability between practitioners — both in how they performed the tests and in the outcomes they recorded. Putting this together, I was underwhelmed by the lack of rigor and reproducibility. To be honest, I was often underwhelmed by the therapeutic results that followed, too.
Later, I learned that standardization is important in many areas, but when it comes to applied physiology and anatomy, it’s not always helpful unless it’s held within an intelligent framework. The issue wasn’t the tests themselves, but how they were often applied — linearly, and with tunnel vision. It’s not a matter of being an expert anatomist; what matters is the ability to hold multiple inputs at once while remaining curious and open. The picture reveals itself when the data can be held and considered as a living whole.
The living body is far different from the two-dimensional images we study or the cadavers we dissect. Life adds fluidity — physical properties that fundamentally change the nature of the mechanical system, primarily through fluid dynamics.
The hip capsule, for example, isn’t a perfectly enclosed fluid system, but it’s close enough that Pascal’s Law applies: if pressure increases within the capsule, that pressure distributes evenly in all directions. The region that “pays” for that increased pressure is wherever the capsule is most vulnerable — where positional tensioning and tissue health are compromised. These vulnerabilities often arise from differences in vascularity, metabolism, or innervation.
So when we assess the hip, we’re not truly assessing where pressure builds too much; we’re assessing how the area responds — if tension, tissue integrity, or movement coherence are lacking.
Before diving into specific assessments, let’s ground ourselves in the foundational principles that help us visualize how the hip actually moves within the socket — and how to approach assessment with that understanding. This framework will help you make sense of what you feel when you assess or move your own hips.
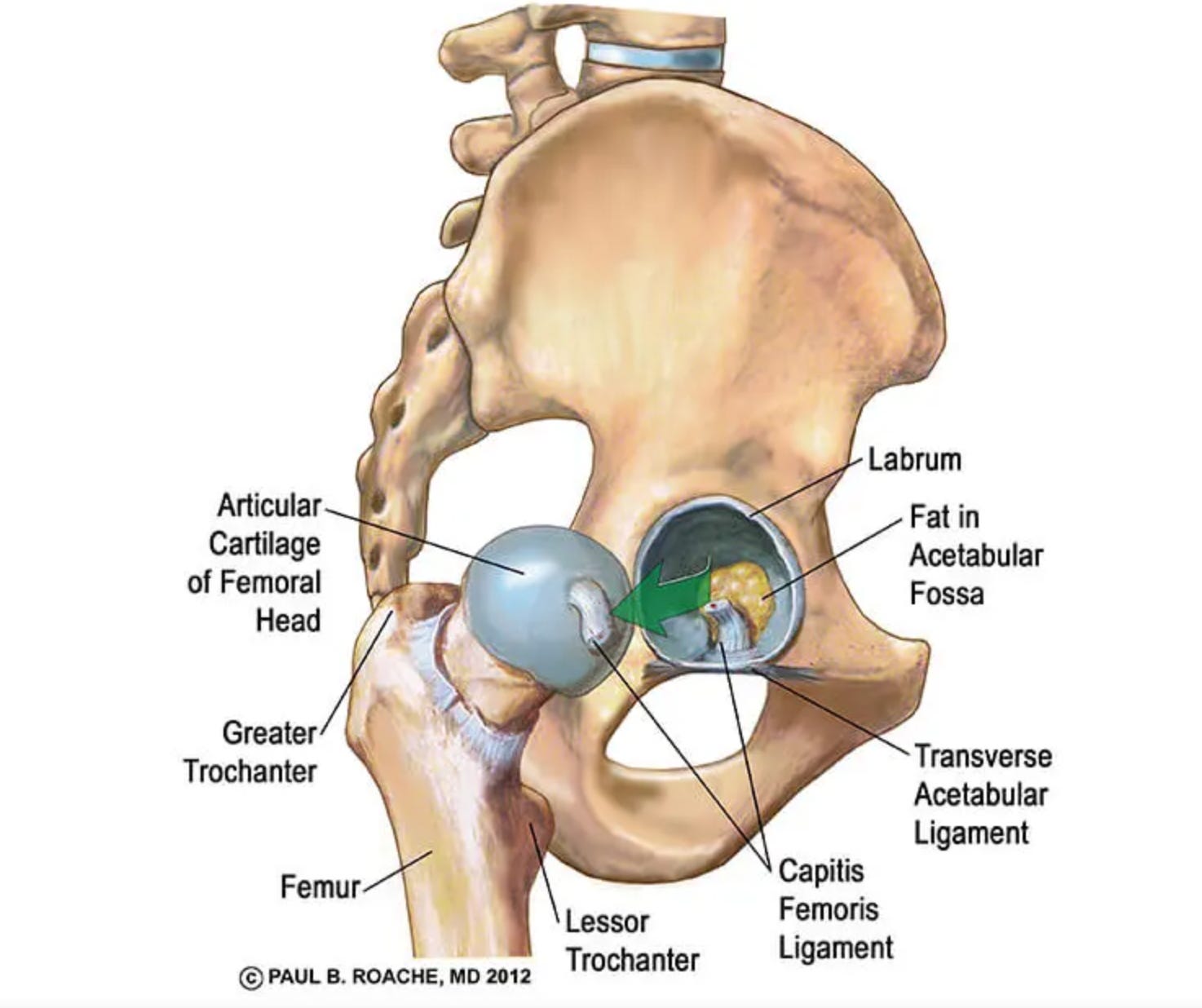
(Below is an image from TeachMeAnatomy illustrating the femoral head within the acetabulum.)
Glide and Roll
The head of the femur “wants” to move in the same direction as the femur itself. When the leg moves forward, the head of the femur also wants to move forward. This motion is called a roll.
However, to keep the joint centered, there must be a counterbalancing motion — a glide — in the opposite direction. So while the leg rolls forward, the head of the femur ideally glides slightly backward within the acetabulum.
This opposing relationship — simultaneous roll and glide — is what keeps the hip joint centered and efficient through its range. Both motions can become disturbed, leading to imbalance, instability, or pain.
End-Range Feel
The end range is the last portion of movement before tension stops you. For example, as you bring your leg forward into flexion, the final 5% of motion — where you feel a limit — is the end range.
Pay attention to the quality of this end feel.
Does it feel abrupt and hard, like running into a wall?
Does it come to a smooth, gradual stop?
Does it jerk, pop, or shift unexpectedly?
Ideally, the leg should decelerate smoothly and naturally, suggesting the capsule and surrounding tissues are maintaining balanced tension. A hard or uneven end feel indicates that the joint capsule or supporting anatomy is not maintaining structural coherence through the movement.
Mid-Range Feel
While end-range issues are more obvious, disturbances can also appear in the mid-range of motion — where the joint should glide most freely. Movement here should feel smooth in all directions. Clicking, popping, pinching, or soreness in mid-range motion indicates compromised hip mechanics and often precedes more serious dysfunction.
Total Range
Looking at total joint range provides a broader picture. Sometimes imbalance shows up not as pain or restriction, but as diffuse fatigue, soreness, or underperformance.
For instance, if the hip has excellent flexion (forward), abduction (out to the side), adduction (inward), and rotation (both internal and external), but poor extension (backward), that asymmetry is meaningful. It suggests the hip capsule and surrounding soft tissue have adapted to an imbalanced tension pattern. Perhaps the glide or roll are disturbed. Restricted motion in any direction indicates a challenge to joint centering.
Important Considerations
a. Side-to-side mobility: Are both hips roughly equivalent in range and feel?
b. Systemic balance: Do the hips reflect the same general quality of mobility as the rest of the body?
c. Expected ranges of motion:
Flexion (leg forward) 120°–130°
Extension (leg backward) 10°–20°
Abduction (leg out to side) 40°–45°
Adduction (leg toward midline) 20°–30°
Internal Rotation 20°–60°
External Rotation 30°–60°
Ratios between these movements matter — disproportionate ranges often reveal compensatory patterns.
Discomfort and Practical Testing
I remember when my left hip was sore thinking it was a bit silly to perform a dozen tests. I’d tell the physiotherapist, “The inside, lower part of my hip is sore. It feels like it’s pinched” After 15 minutes of testing, they’d say, “It’s inflamed and impinged.” Yes — I know. That’s why I’m here.
I say this because it’s useful to maintain this no-nonsense perspective when working with the body. If something hurts — something is wrong. But with that said, comprehensive testing can help identify why discomfort occurs. The inner hip may hurt due to a local impingement, excessive tension from a lateral shift of the femoral head, sacroiliac dysfunction, fascial torsion inside the pelvis, or even knee misalignment. Intelligent testing helps trace the root cause.
Still, discomfort alone is often enough to indicate a hip-centering problem. For example, even if the hip moves forward due to a previous ACL injury, the adaptation can still be improved. The body doesn’t have to compensate for one problem by creating another — we can guide it to adapt more intelligently.
Assessments
(I apologize for my raspy voice in the recordings from my head cold.)
The following assessments help you understand different aspects of hip centering and related relationships:
Modified Thomas Test — assesses hip flexor length and anterior hip tension.
Lie on a table and hold your knee into your chest. Let the other knee drop down. We’re looking at 3 things here.
a. Do you feel pinching in the knee brought to the chest? (this is a bonus input)
If so, there is something going on with hip centering in flexion on the same side.
b. How low is the leg that’s dropping off the table?
c. Is the knee relaxed at a 90 degree angle?
Ideally, it should hang off the table with the knee flexed at 90 degrees.
If you notice both restriction in bringing your knee to chest AND your leg is lifted off/the knee want to extend to less than 90 degrees, there is a good change you have some anterior impingement going on and the head of the femur is not ideally centered.
Passive Range of Motion (ROM) — evaluates smoothness, end feel, and joint glide.
The video takes you through a range of movements of the hip. Notice pinching, hard end feels, jerky end feels and asymmetries.
Posterior Glide Test — checks the femoral head’s posterior mobility.
Start with your knee up to 90 degrees, perpendicular to the floor. Lying on your back, use your arms to pull your femur directly down to floor as if it could push through your glutes. Notice if there is movement or if it feels like you are pushing against an entirely rigid structure. The movement should be small but present. Comparing your two sides can help paint a picture.
Hip Hinge & Squat — examines functional integration and load control.
Sometime poor hip centering is a functional problem. This means that the pattern of activation is leading to poor micro-movement control. Overtime this can lead to structural changes. Notice if your able to hinge and squat while keeping a long neutral spine. Do the hips allow for the movement? Do they feel compressed?
90/90 Walks — reveals rotational control and pelvic balance.
Notice in this movement if the hips are able to move freely without pain, popping or a harsh end- feel. If not, it indicates a joint centering imbalance likely in relationship to the rotators and the pelvis.
SIJ Assessment — evaluates sacroiliac joint contribution to hip positioning.
This is a general assessment for the balance of tension over the Sacro-Iliac joint. Notice discrepancies from side to side, freedom of movement and ease in maintaining a stable sacrum.
Putting it all together
Now that you’ve gone through these 6 assessments, you may be wondering — what does it all mean? I may sound like a broken record at this point, but I want you to be noticing and thinking in generalities. Keep you “big picture” brain engaged. Notice the patterns. Here’s what I found and a look into my thinking process.
Assessment results
Left side Modified Thomas Test restricted
Left side hard end feel in internal rotation
Left side more abduction
Right side soreness in full flexion
Right side restricted posterior glide test
Slight impingement right side squat
90/90 Walks popping on left side
SIJ restricted left side
Any patterns?
Yes! Everything on the left side that is challenges has to do with moving the femur forward. (Note that internal rotation is a forward motion and external is a backwards)
The right side pattern is that flexion (forward movement) cause discomfort and that there is restriction in moving the femur backwards.
Takeaway
I caution against moving into any assumptions from these results along the line of “the right hip is too tight in the front” or “the left is too tight in the back”. Instead, I would simply be aware of the discrepancy and note that both sides are not ideally centered. Furthermore, working on my hip centering will be helpful.
It’s perhaps not the most exciting takeaway, but at this stage, it offers the greatest openness for genuine data collection. As I continue with other assessments, exercises, and stretches, the pattern will naturally reveal itself and deepen. Trusting this organic process is an essential part of health.
It can be difficult to remain in that curious, open space — we tend to settle on “nodes,” points of perceived certainty that feel safe. But once we decide we understand the system, curiosity narrows. Our perception becomes filtered, and we start looking only for evidence that confirms our hypothesis.
Finding the true root cause — the primary lesion — is an art that requires patience, humility, and the willingness to keep seeing with fresh eyes.
Amy,
Holy. Holy. Holy.
Gratitude for your translation.
I have saved your post to read again and restack.🫶🏼
Hi Amy,
Last year I got a virus and a few weeks later developed an autoimmune condition called polymyalgia rheumatica which is medical speak for we don't what the hell this is. The initial symptoms were severe stiffness in the hips in the morning which would get better later in the day. I'm OK now after having to take cortico-steroids for a while to reduce inflammation, but I went to a physio I hadn't been to before at the time. He did many of these tests on me and said that I needed two hip replacements. Fortunately I ignored him and my regular physio and I agreed after some treatments that it was something systemic that he couldn't help. I diagnosed myself from the internet and informed my General Practitioner who agreed, did blood tests and put me on the steroids. My point is that the tests were useless without understanding the broader context, which I think is your point, yes?